Influenza (flu) is a universally common epidemic illness caused by several subtypes of type A or by type B influenza virus. (Type C influenza virus exists and produces a mild respiratory illness but is not believed to cause epidemics.) The most common subtypes of influenza A are H1N1 and H3N2. A subtype of avian influenza A that emerged in Asia (H5N1) produces infrequent but often fatal human illness. A swine-origin influenza A (H1N1) virus outbreak, beginning in March and April of 2009, reinforces that interspecies transmission of human and animal influenza A viruses and subsequent reassortment are possible and occur, resulting in new viruses that may spread to humans and even easily between humans.
Current flu season: Per the Centers for Disease Control and Prevention (CDC), as of April 6, 2024, seasonal influenza activity remains elevated but continues to decrease nationally in the United States. Both influenza A and influenza B are being reported by public health laboratories. Coinfection with influenza A or B viruses, respiratory syncytial virus, and SARS-CoV-2 can occur.
Influenza is highly contagious and is spread by aerosol droplets. The incubation period is 1-4 days, but it becomes contagious 1 day prior to the onset of symptoms. The mortality rate of influenza is low but tends to be higher in the elderly and the immunocompromised. Flu activity usually peaks in February.
Influenza presents with classic flu-like illness consisting of the sudden onset of fever, malaise, sore throat, nonproductive cough, myalgias, headache, and nasal congestion. Chills are common, as are nausea and vomiting in children. After 48 hours, cough may increase and produce sputum. There may be associated dyspnea and/or mild-to-moderate pleuritic chest pain. Upon physical examination, unilateral or bilateral inspiratory rales may be appreciated or diminished breath sounds. Pregnant individuals are at increased risk for severe illness from influenza.
Most viruses that affect the respiratory tract can cause a rash, flu included (see viral exanthem).
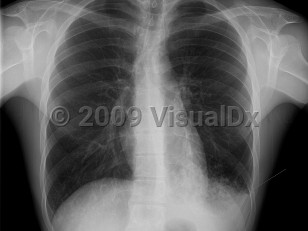
The most common pulmonary complication of influenza is secondary bacterial pneumonia. This diagnosis can be determined by patient history. This can occur up to 2 weeks after the initial symptoms and includes recurrence of fever, chills, pleuritic chest pain, and productive cough. Many bacteria may be the culprit, but the most common are pneumococci. Staphylococcus aureus has also been implicated in children; there has been an increase in the number of deaths in which both influenza and pneumonia or bacteremia due to S aureus were identified.
Primary viral pneumonia is the complication responsible for the most influenza-related deaths. Those with pre-existing cardiopulmonary disease or who are pregnant are at the greatest risk. The initial clinical presentation is the same, but dyspnea increases in severity. Productive cough may be blood tinged. Massive hemoptysis has been reported. When severe, there may be profound respiratory distress with tachypnea, tachycardia, and cyanosis. Rales and wheezes will spread throughout the chest from the lower lung.
The Spanish flu pandemic of 1918 was particularly virulent, killing over 20 million people worldwide. With present day biotechnology, it would be possible to produce an influenza virus weapon with traits of both the H5N1 and the 1918 influenza viruses. As a weapon, influenza could be released as an aerosol.
Note: In 2022 and 2023, pediatric invasive group A streptococcal (iGAS) infections and noninvasive group A streptococcal infection cases have been associated with respiratory infections due to influenza, among other viruses. Concurrent or preceding viral infections, including varicella (chickenpox), may increase risk for iGAS infection. Severe outcomes of iGAS infections include necrotizing fasciitis, streptococcal toxic shock syndrome, and death.
Influenza in Infant/Neonate
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
J10.1 – Influenza due to other identified influenza virus with other respiratory manifestations
SNOMEDCT:
6142004 – Influenza
J10.1 – Influenza due to other identified influenza virus with other respiratory manifestations
SNOMEDCT:
6142004 – Influenza
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Reviewed:09/12/2022
Last Updated:04/11/2024
Last Updated:04/11/2024
 Patient Information for Influenza in Infant/Neonate
Patient Information for Influenza in Infant/Neonate
Premium Feature
VisualDx Patient Handouts
Available in the Elite package
- Improve treatment compliance
- Reduce after-hours questions
- Increase patient engagement and satisfaction
- Written in clear, easy-to-understand language. No confusing jargon.
- Available in English and Spanish
- Print out or email directly to your patient
Upgrade Today