Seborrheic dermatitis presents in infants as a self-limited eruption caused by persistent maternal androgens, or in adults, after adrenarche. Up to 5% of adults are affected by seborrheic dermatitis, and the condition is particularly common after the fifth or sixth decades.
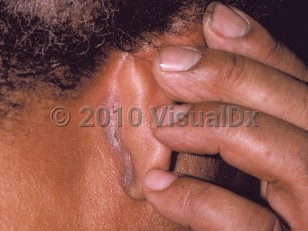
Clinical presentations of seborrheic dermatitis are widely varied, ranging from simple "dandruff" to fulminant rash. There is often dryness, pruritus, erythema, and fine, greasy scaling in characteristic sites, such as the scalp, eyebrows, glabella, nasolabial folds, the beard area, upper chest, external ear canal, posterior ears, eyelid margins (blepharitis), and intertriginous areas. Anogenital involvement has also been reported. One or multiple sites may be involved. In persons with darker skin phototypes, the involved areas may be hypopigmented or hyperpigmented. These pigmentary changes may persist after treatment.
Stress may exacerbate the condition. In immunocompromised persons and those with neurologic conditions, such as Parkinson disease or stroke, seborrheic dermatitis may be severe and recalcitrant.
Since seborrheic dermatitis is such a common disorder, it has been difficult to associate it with specific medications. However, there are some published associations of medications causing, triggering, or exacerbating the condition (see Drug Reaction Data table).
Even with treatment, seborrheic dermatitis tends to be a chronic condition, and remissions and exacerbations are expected. Seborrheic dermatitis is often better in summer months and worse in the winter.
Immunocompromised patient considerations:
- Seborrheic dermatitis is more common and more severe in persons infected with the human immunodeficiency virus (HIV). It may regress with highly active antiretroviral therapy, but remissions and exacerbations can be expected.
- Seborrheic dermatitis is also often seen in patients with Parkinson disease. The course is chronic and relapsing and may be difficult to treat.
- Associated Pityrosporum folliculitis may be seen in immunocompromised patients.

 Patient Information for
Patient Information for